Perceptual Learning for Amblyopia: How Practice Retrains the Adult Brain
What perceptual learning is, how Gabor patch training and contrast sensitivity exercises retrain the visual cortex, and what the clinical evidence shows for adults with amblyopia
What Is Perceptual Learning?
Perceptual learning refers to a long-lasting improvement in the ability to perform a specific sensory discrimination task that results from repeated practice. It is not about learning new facts or concepts, it is about the brain becoming better at seeing fine differences through experience. In the context of vision, perceptual learning means that with structured, repeated exposure to carefully controlled visual stimuli, the brain's visual cortex can sharpen its ability to detect subtle differences in orientation, contrast, spatial frequency, and position.
This is fundamentally different from improving vision through optical correction (glasses or contact lenses) or surgery. Perceptual learning targets the neural processing that happens after the eye captures an image, it trains the brain to interpret visual information more accurately. For people with amblyopia (lazy eye), where the brain has learned to suppress or poorly process input from one eye, perceptual learning offers a way to directly retrain the affected neural pathways.
The most widely used stimulus in perceptual learning research is the Gabor patch, a sinusoidal grating (striped pattern) multiplied by a Gaussian envelope that fades the pattern smoothly toward the edges. Gabor patches are ideal for this purpose because they activate specific populations of neurons in the primary visual cortex (V1) that are tuned to particular orientations and spatial frequencies. By presenting Gabor patches with precisely controlled parameters, researchers, and now therapy apps, can target the exact neural circuits that need retraining.
For a deeper explanation of Gabor patches and their parameters, see our dedicated guide: Amblyopia Treatment by Gabor Patches.
The Discovery That Changed Amblyopia Treatment, Adult Brain Plasticity
For much of the 20th century, the dominant view in vision science was that amblyopia could only be treated effectively during a critical period in early childhood. The assumption was that after age 7-10, the visual cortex had finished its development and was no longer capable of significant change. Adults with amblyopia were routinely told that nothing more could be done, that the vision loss was permanent.
This view has been substantially overturned. A growing body of research, beginning in the late 1990s and accelerating through the 2000s, has demonstrated that the adult visual cortex retains significant neuroplasticity. Perceptual learning studies have repeatedly shown that adults with amblyopia can achieve measurable improvements in visual function through structured training, even decades after the critical period.
A landmark review by Levi and Li (2009) in Vision Research synthesized evidence from multiple studies and concluded that perceptual learning can improve visual acuity, contrast sensitivity, and spatial resolution in adults with amblyopia. The authors noted that improvements were not limited to the trained task but often generalized to untrained visual functions, suggesting genuine neural reorganization rather than simple task familiarity.
Zhou and colleagues (2006) demonstrated that adults with anisometropic amblyopia (mean age 21 years) who completed 10 daily sessions of Gabor patch orientation discrimination training showed significant improvements in visual acuity, an average gain of about 1.5 lines on a standard eye chart. Importantly, these gains were retained at a 5-month follow-up, indicating lasting neural change.
Polat and colleagues (2004) showed that adults with amblyopia who trained on a lateral-masking contrast detection task for 30 sessions over several months improved not only on the trained task but also showed improvements in visual acuity and contrast sensitivity that generalized beyond the trained stimulus parameters. This study, published in the Proceedings of the National Academy of Sciences, was among the first to demonstrate that perceptual learning could produce clinically meaningful improvements in adult amblyopia.
The mechanism behind this adult plasticity appears to involve both bottom-up changes in early visual cortex (V1), where neurons become more sensitive to the trained stimulus features, and top-down attentional modulation that helps the brain allocate more processing resources to input from the amblyopic eye. Functional imaging studies (fMRI and VEP) have shown that perceptual learning increases cortical responses to stimuli presented to the trained amblyopic eye and reduces the neural suppression that characterizes amblyopia.
How Perceptual Learning Works, Contrast, Crowding, and Orientation Tasks
Perceptual learning for amblyopia typically involves one or more of the following task types, each targeting a specific aspect of visual processing that is impaired in amblyopia:
Contrast Detection and Discrimination
The amblyopic eye typically has elevated contrast thresholds, it needs stronger contrast to detect a stimulus compared to the non-amblyopic eye. Perceptual learning tasks that require detecting or discriminating low-contrast stimuli can push these thresholds downward. In practice, this means starting with high-contrast targets that are easy to see and gradually reducing contrast as the visual system adapts. This is one of the most effective difficulty levers in perceptual learning, and it is the primary mechanism used in the FlankerScene exercise in Lazy Eye Games & Exercises, where the central target's contrast decreases progressively across 24 levels while flanker contrast remains at 100%.
Orientation Discrimination
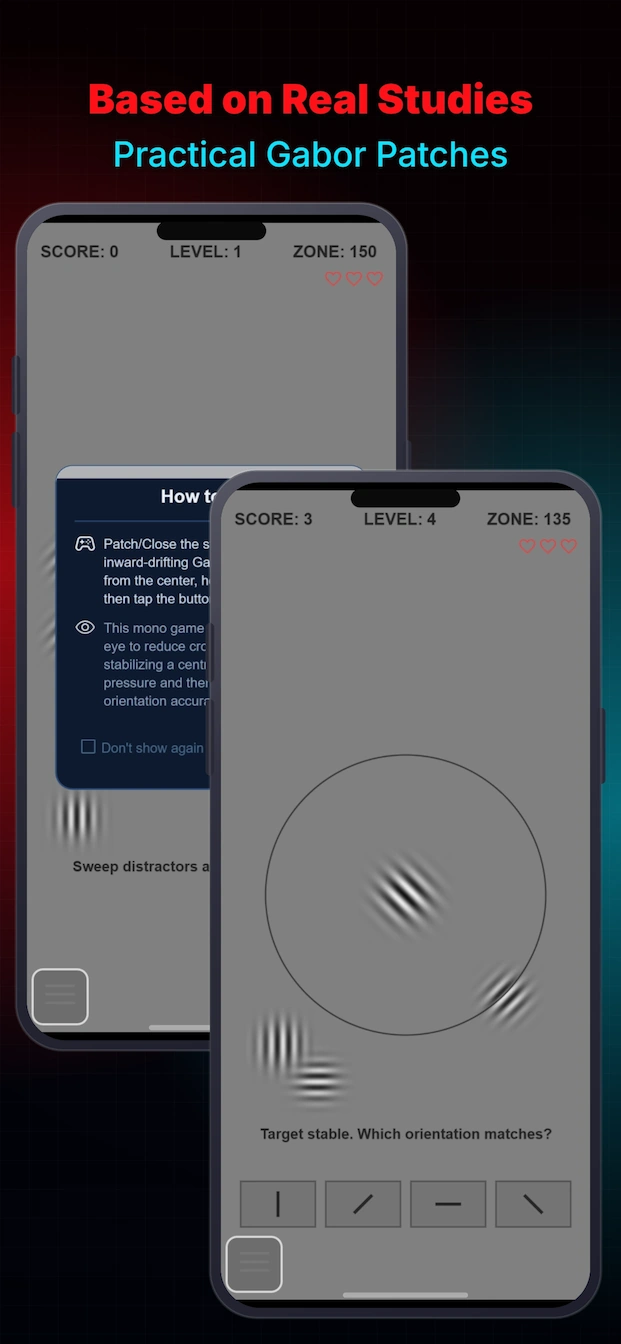
Telling whether a Gabor patch is tilted slightly clockwise or counterclockwise is one of the cleanest perceptual learning tasks. The brain's orientation-selective neurons in V1 can be trained to finer and finer discriminations through repeated practice. In the GaborMatchScene exercise, the patient studies a target Gabor patch and selects the matching option from a grid of decoys. As levels progress, the orientation difference between the target and decoys shrinks, and contrast decreases, making the discrimination progressively harder.
Crowding Reduction
Crowding is a hallmark deficit in amblyopia: the ability to identify a target is severely impaired when it is surrounded by nearby distractors, even when the target itself is large enough to be seen in isolation. Perceptual learning tasks that require identifying a target in the presence of flanking stimuli can reduce the crowding zone. The Gabor Crowding game (GaborCrowdingScene) directly targets this: the player sweeps inward-drifting Gabor distractors away from a central target, holds the target stable, and then identifies its orientation. The FlankerScene exercise also targets crowding by progressively moving the flankers inward, increasing collinear masking pressure as the level advances.
Contour Integration
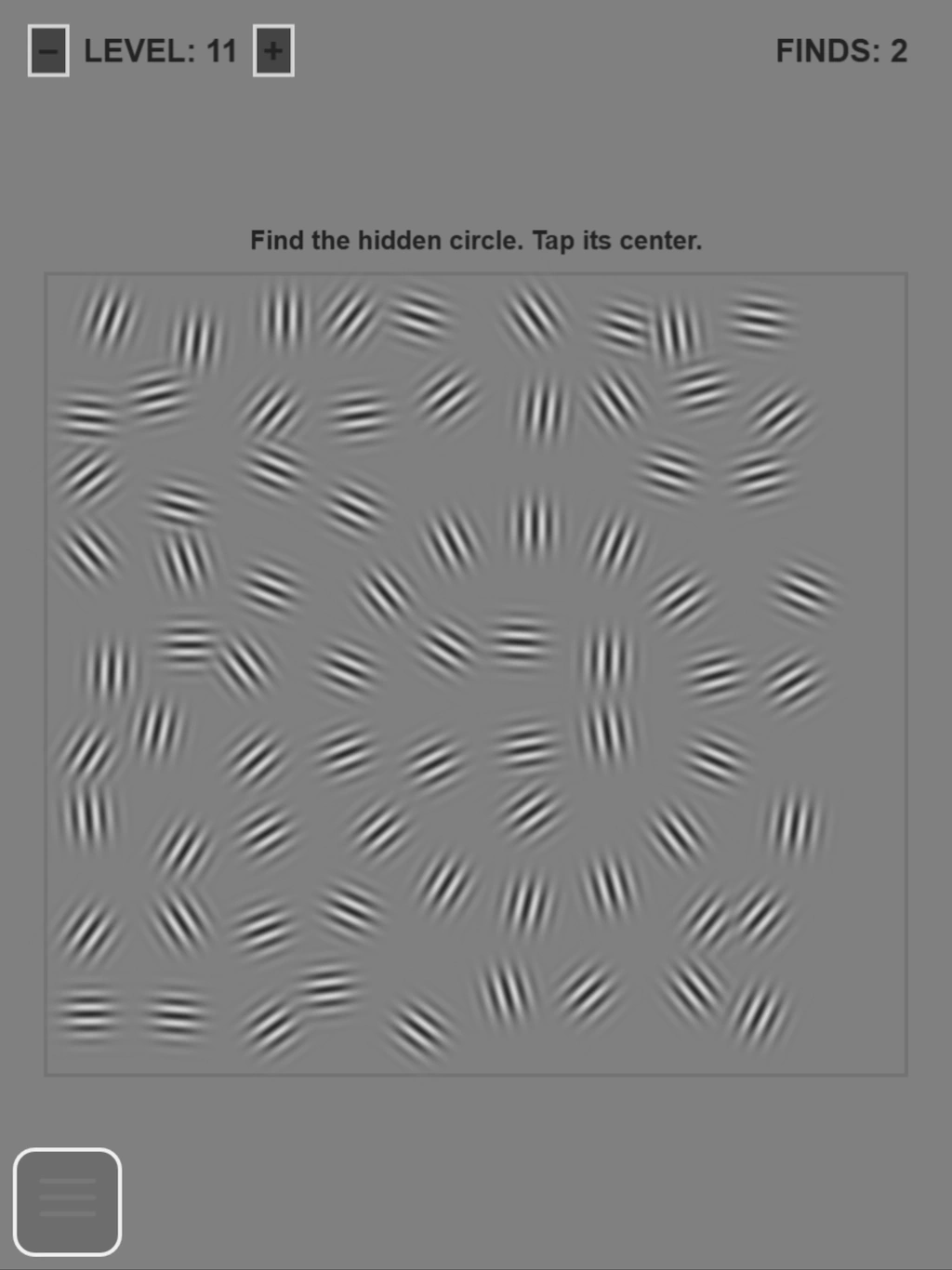
Amblyopia also impairs the ability to integrate local visual elements into a global percept, for example, seeing a shape made of aligned Gabor patches embedded in a field of randomly oriented patches. The GaborContourScene exercise trains this skill by hiding a circular contour made of tangent-aligned Gabor patches within a noisy field of identical patches with random orientations. The patient must segment the full shape and tap its centre. Difficulty increases through higher noise density, tighter contour spacing, and orientation jitter on the contour elements.
Lateral Masking (Polat-Style Training)
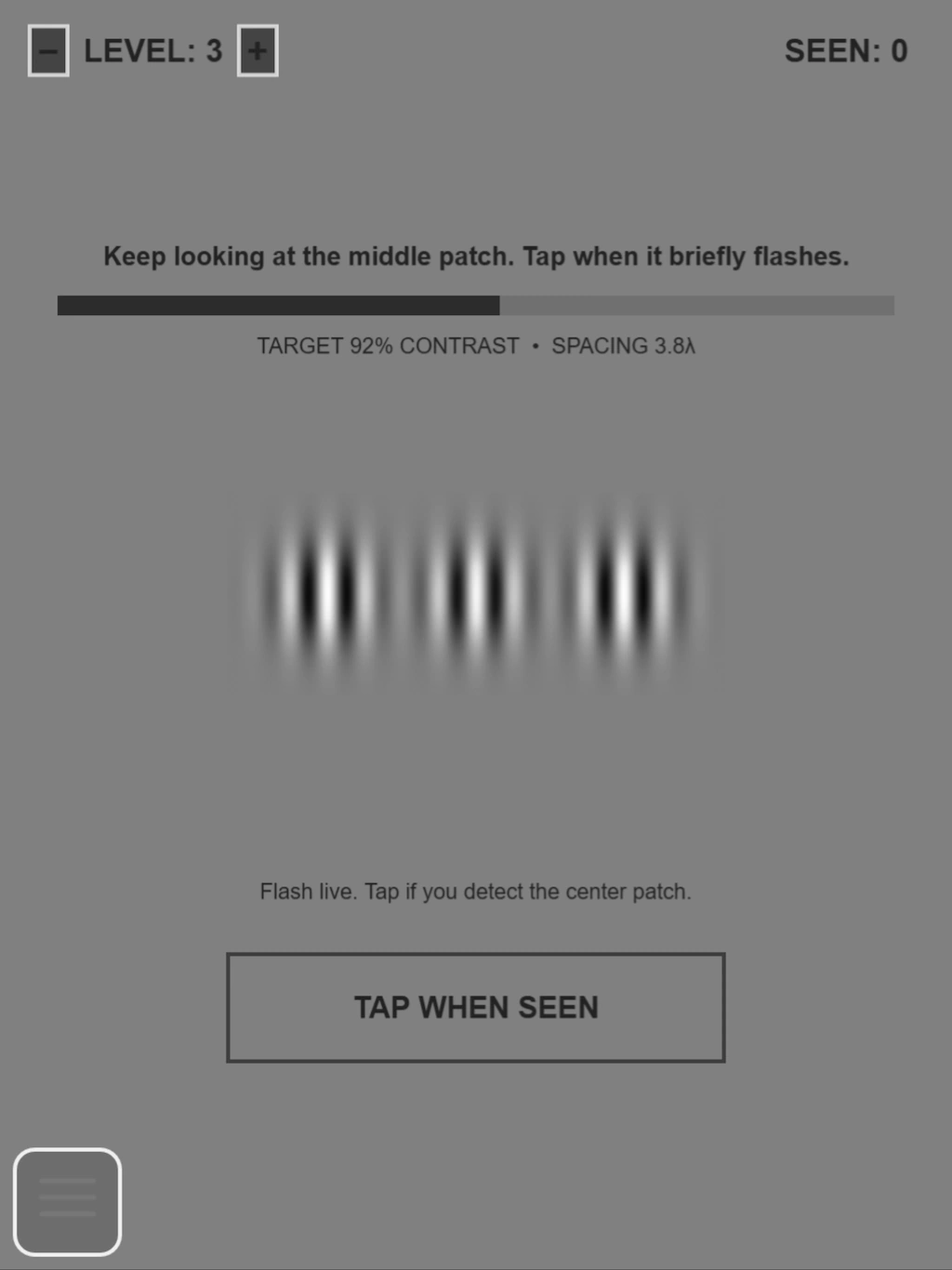
A well-established perceptual learning paradigm developed by Polat and colleagues involves detecting a low-contrast Gabor target presented between two higher-contrast flankers. In normal vision, collinear flankers can actually improve target detection (lateral facilitation), but in amblyopia this facilitation is reduced or absent. Training on this task can restore lateral interactions in the visual cortex. The FlankerScene exercise in the app is built directly on this paradigm, and the Gabor Constellation game adapts it into an arcade format where the player swipes when a faint midpoint target flashes between two darker flankers.
Key Parameters Used in Gabor-Based Perceptual Learning
The app's Gabor exercises are built on a centralized parameter engine that controls every aspect of the stimulus with scientific precision:
- Spatial frequency, stripe density, measured in cycles per pixel or cycles across the patch. Higher spatial frequencies are more challenging for the amblyopic eye and are a key training dimension.
- Contrast, how strongly the stripes deviate from the neutral gray background. Contrast is the primary difficulty lever, reduced progressively as the patient improves.
- Orientation, the angle of the stripes, normalized to the [0, π) range. Orientation discrimination is trained by shrinking the angular difference between target and decoys.
- Sigma (envelope width), controls the Gaussian envelope radius, determining how many visible stripes appear in the patch.
- Phase, the shift of the stripe pattern along the carrier axis, kept fixed within a round so the patient solves the intended discrimination task.
- Cycles across patch, a size-normalized frequency representation that preserves apparent stripe density when patches are rendered at different sizes, ensuring fair comparison between target and options.
All Gabor stimuli are procedurally generated at runtime through the centralized utility, with anti-aliasing guards, amplitude headroom computation (to prevent luminance clipping), and mean luminance matching to the neutral gray background. This ensures the stimulus is scientifically valid and not merely decorative.
What Does the Research Show?
The clinical evidence for perceptual learning in amblyopia has accumulated over more than two decades. Below is a summary of key findings from peer-reviewed studies. The picture is encouraging but also nuanced, results vary by study design, amblyopia type, and individual patient factors.
| Outcome | Typical Finding | Key Studies |
|---|---|---|
| Visual Acuity Gains | 1-2.5 lines (logMAR) improvement in the amblyopic eye after 10-30 training sessions | Zhou et al. (2006); Polat et al. (2004); Levi & Li (2009) review |
| Contrast Sensitivity | Significant improvement at multiple spatial frequencies, often generalizing beyond trained frequencies | Polat et al. (2004); Zhou et al. (2006); Huang et al. (2008) |
| Crowding Reduction | Reduced crowding zone and improved target identification in clutter | Levi, Song & Pelli (2007); Hussain et al. (2012) |
| Generalization | Improvements often transfer to untrained orientations, spatial frequencies, and even untrained tasks (e.g., reading) | Polat et al. (2004); Zhou et al. (2006); Astle, Webb & McGraw (2011) |
| Long-Term Retention | Gains retained at 5-12+ months post-training in most studies that measured retention | Zhou et al. (2006), 5 months; Huang et al. (2008), 12 months |
| Neural Correlates | Increased VEP amplitudes and fMRI BOLD responses in V1 for the trained eye; reduced interocular suppression | Zhang et al. (2014); Bao et al. (2008); Ding & Levi (2011) |
Important Caveats and Variability
While the overall evidence is positive, it is important to be honest about the limitations and variability in the research:
- Sample sizes in most perceptual learning studies are relatively small (typically 10-30 participants), which limits the statistical power and generalizability of findings.
- Individual variability is substantial. Some patients show large improvements while others show minimal change. The factors that predict who will benefit most are not yet fully understood.
- Amblyopia type matters. Patients with anisometropic amblyopia (different refractive errors between eyes) may respond differently than those with strabismic amblyopia (eye misalignment) or mixed types.
- Home-based translation of laboratory findings is an active area of research. Most published studies were conducted in controlled laboratory or clinic settings with supervised sessions. The effectiveness of unsupervised home-based training, while promising, is less thoroughly documented.
- Optimal dosing, the ideal session duration, frequency, and total number of sessions, has not been firmly established. Studies have used widely varying protocols, from 10 sessions over 2 weeks to 30+ sessions over several months.
These caveats do not diminish the significance of the findings, but they underscore that perceptual learning is a developing therapeutic approach rather than a settled, standardized treatment. It is best understood as a complementary tool within a broader vision therapy plan, not a standalone cure.
Perceptual Learning vs Dichoptic Training vs Patching
Perceptual learning, dichoptic training, and traditional patching target different mechanisms in amblyopia. Understanding the differences helps clarify why a combined approach may be more effective than any single method.
| Aspect | Perceptual Learning | Dichoptic Training | Patching (Occlusion) |
|---|---|---|---|
| Mechanism | Repeated discrimination practice with controlled stimuli (Gabor patches) to retrain low-level visual processing | Presenting different images to each eye simultaneously to reduce interocular suppression and train binocular fusion | Occluding the stronger eye to force exclusive use of the amblyopic eye |
| Eye(s) trained | Monocular, amblyopic eye alone (strong eye patched) | Binocular, both eyes receive complementary input | Monocular, amblyopic eye alone |
| Equipment needed | Eye patch (no 3D glasses) | Red-cyan anaglyph 3D glasses | Adhesive eye patch |
| Primary target | Contrast sensitivity, orientation discrimination, spatial resolution, crowding reduction | Binocular fusion, anti-suppression, stereopsis (depth perception) | Visual acuity in the amblyopic eye |
| Typical setting | Structured sessions with controlled stimuli; increasingly available in home-based apps | Interactive games or exercises; well-suited to home use | Passive wear during daily activities |
| Evidence for adults | Strong, multiple studies show acuity, contrast sensitivity, and spatial vision improvements in adults (Levi & Li, 2009; Zhou et al., 2006; Polat et al., 2004) | Moderate to strong, studies show binocular function and stereoacuity improvements in adults (Hess et al., 2012; Vedamurthy et al., 2015) | Limited, some acuity gains in adults but poor compliance and limited binocular benefit |
| Compliance challenge | Low to moderate, requires active engagement but sessions are typically short (5-15 minutes) | Low, sessions are engaging and gamified | High, long wear times, skin irritation, social stigma, boredom |
The three approaches are not mutually exclusive. In fact, they may be synergistic: perceptual learning improves the amblyopic eye's basic visual processing capacity, dichoptic training teaches the brain to use both eyes together, and patching (when appropriate) provides additional monocular stimulation. The Lazy Eye Games & Exercises app is designed around this complementary model, offering both dichoptic activities (with anaglyph glasses) and monocular perceptual learning exercises (no glasses needed, using an eye patch).
For a detailed explanation of dichoptic training, see our guide: Dichoptic Training for Amblyopia: How It Works, Evidence, and Practicing at Home.
How Lazy Eye Games & Exercises Applies Perceptual Learning
The Lazy Eye Games & Exercises app implements perceptual learning through a dedicated set of monocular Gabor-based activities. These are designed to be used with the strong eye patched or closed, no 3D glasses are required. The app's perceptual learning activities fall into two categories:
Clinical-Grade Exercises
These are structured, stress-free exercises that follow established perceptual learning paradigms from the research literature:
- Gabor Match, The patient studies a target Gabor patch and selects the matching option from a grid of decoys. Difficulty increases through smaller orientation and spatial frequency differences between target and decoys, and through reduced contrast. Uses 25 levels with grid sizes from 3×1 up to 4×3.
- Gabor Flanker, Based on the Polat lateral-masking paradigm. The patient detects a faint central Gabor target presented between two high-contrast collinear flankers. Contrast of the central target decreases and flanker spacing tightens across 24 auto-advancing levels.
- Gabor Contour, The patient searches a noisy field of Gabor patches for a hidden circular contour made of tangent-aligned patches. Trains global contour integration and figure-ground segregation across 12 levels.
- Gabor Float, The patient tracks drifting Gabor patches across the screen, training smooth pursuit and sustained attention with the amblyopic eye.
- Gabor Flash, The patient identifies briefly flashed Gabor stimuli, training rapid visual processing and saccadic accuracy.
- Gabor Spin, The patient discriminates the orientation of rotating Gabor patches, training dynamic orientation processing.
- Gabor Axes, A 30-level clinical progression from contrast detection to crowding, providing a structured perceptual learning curriculum.
- Ball Tracking, Combines Gabor stimuli with smooth pursuit tracking for integrated perceptual and oculomotor training.
Gamified Perceptual Learning
To improve engagement and compliance, the app also wraps perceptual learning mechanics into arcade-style games:
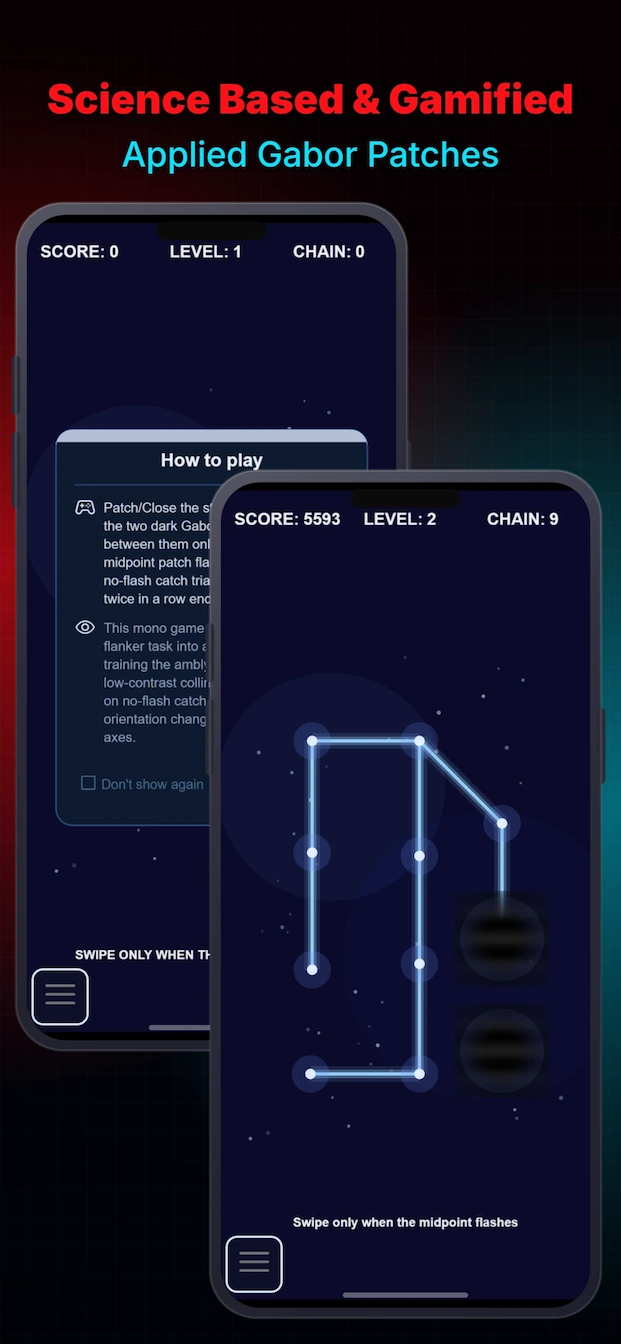
- Gabor Constellation, An arcade lateral-masking game where the player swipes when a faint midpoint target flashes between two darker Gabor flankers. Based on the Polat et al. (2004) paradigm.
- Gabor Crowding, The player sweeps inward-drifting Gabor distractors away from a central target, holds it stable, and identifies its angle. Trains crowding tolerance, fixation stability, and orientation discrimination together.
- Gabor Memory, Classic memory matching with procedurally generated Gabor patch pairs, training orientation and spatial frequency discrimination through a familiar game format.
- Gabor Diff, Timed difference search across paired Gabor grids, training rapid discrimination of subtle parameter differences.
- Gabor Birdy, Flappy-style gameplay with Gabor patch obstacles, training sustained attention and rapid visual processing.
- Gabor Grid, Flow-grid puzzle connecting Gabor patch endpoints with difficulty-scaled visual spacing.
Adaptive Difficulty and Progress Tracking
All perceptual learning activities in the app use adaptive difficulty mechanisms inspired by the staircase procedures used in research. As the patient improves, the app automatically adjusts:
- Contrast reduction, the primary difficulty lever, decreasing progressively to push contrast sensitivity
- Orientation discrimination narrowing, decoy patches become more similar to the target
- Crowding increase, flankers move closer to the target, increasing lateral masking pressure
- Spatial frequency increase, stripe density increases, challenging the amblyopic eye's resolution limits
The app's VisionProfileScene tracks perceptual learning progress over time, showing a 3-axis radar chart that includes the Perceptual Learning clinical category alongside Anti-Suppression, Fusion Training, and Stereopsis. This allows patients and their eye care professionals to see how monocular training is progressing alongside binocular training.
What to Expect, Consistency and Realistic Timelines
Perceptual learning is not a quick fix. The improvements documented in research studies required consistent, repeated practice over weeks or months. The key findings on dosing from the literature include:
- Zhou et al. (2006) used 10 daily sessions of approximately 30-40 minutes each over two weeks, with measurable acuity gains appearing after about 5-7 sessions.
- Polat et al. (2004) used 30 sessions over several months, with improvements continuing to accumulate across the training period.
- Most studies report that improvements are gradual and continue to develop even after training ends, suggesting that consolidation of neural changes takes time.
- Consistency appears to be more important than session length. Shorter daily sessions (10-15 minutes) may be as effective as longer sessions done less frequently.
For home-based training with the Lazy Eye Games & Exercises app, a reasonable expectation is:
- First 1-2 weeks: Familiarization with the exercises and building a daily habit. Most users will not notice significant changes this early.
- Weeks 3-6: Some users begin to notice that tasks that felt difficult at the start are becoming easier. The app's adaptive difficulty will have progressed to harder levels.
- Weeks 7-12: More noticeable improvements in everyday visual comfort, contrast sensitivity, and perhaps visual acuity, though individual results vary widely.
It is important to emphasize that individual results vary and that home-based training has not been studied as extensively as supervised laboratory training. The app is designed to support consistent practice, but it cannot guarantee specific outcomes.
When to See an Eye Care Professional
Perceptual learning is a therapeutic tool, not a substitute for professional eye care. A comprehensive eye examination by an optometrist or ophthalmologist is essential before starting any vision training program. An eye care professional can:
- Diagnose the specific type and severity of amblyopia or binocular vision disorder
- Rule out other conditions that may require different treatment
- Determine whether perceptual learning is appropriate for your specific needs
- Monitor progress and adjust the treatment plan as needed
- Provide guidance on integrating at-home training with in-office vision therapy
If you experience persistent double vision, headaches, eye strain, or sudden vision changes while training, stop and consult your eye care professional before continuing.
For more resources, including books, videos, and professional organizations, see our Recommended Resources page.
Frequently Asked Questions
Can perceptual learning improve vision in adults with amblyopia?
Yes. Multiple peer-reviewed studies have demonstrated that perceptual learning can improve visual acuity, contrast sensitivity, and spatial resolution in adults with amblyopia, including patients who were previously told they were "too old" for treatment. Key studies include Zhou et al. (2006), Polat et al. (2004), and the comprehensive review by Levi and Li (2009). Improvements are typically in the range of 1-2.5 lines on a standard eye chart.
How is perceptual learning different from eye exercises?
Perceptual learning is a specific, scientifically defined phenomenon: practice-driven improvement in sensory discrimination. It is distinct from general "eye exercises" (such as accommodation or vergence exercises) because it targets low-level neural processing in the visual cortex through repeated, controlled stimulation with precisely parameterized stimuli. Perceptual learning tasks are designed to push the brain's sensory processing limits, not to strengthen eye muscles or improve focusing.
Do the improvements from perceptual learning last?
Several studies have reported that perceptual learning gains are retained for months or even years after training ends. Zhou et al. (2006) found that visual acuity improvements were maintained at a 5-month follow-up. Huang et al. (2008) reported retention at 12 months in adult amblyopia patients. This durability suggests that perceptual learning induces lasting neural reorganization in the visual cortex, not just temporary task familiarity.
What is a Gabor patch and why is it used in perceptual learning?
A Gabor patch is a sinusoidal grating (striped pattern) multiplied by a Gaussian envelope that fades the pattern smoothly toward the edges. It is used in perceptual learning because it selectively activates specific populations of neurons in the primary visual cortex (V1) that are tuned to particular orientations and spatial frequencies. This makes Gabor patches an ideal stimulus for targeted training of the neural circuits that are impaired in amblyopia. For a full explanation, see our Amblyopia Treatment by Gabor Patches guide.
How does perceptual learning compare to dichoptic training?
Perceptual learning is monocular (the strong eye is patched) and trains the amblyopic eye's contrast sensitivity, orientation processing, and spatial resolution. Dichoptic training is binocular (both eyes receive different images through anaglyph glasses) and trains the brain to reduce interocular suppression and fuse input from both eyes. The two approaches target different mechanisms and are complementary. The Lazy Eye Games & Exercises app includes both modalities. See our Dichoptic Training guide for more detail.
How long does perceptual learning take to show results?
Research studies typically involve 10-30 training sessions over several weeks. Zhou et al. (2006) used 10 daily sessions over two weeks. Polat et al. (2004) used 30 sessions over several months. Home-based results vary by individual, and consistency of practice appears to be the most important factor. Most studies report measurable improvements after 10-15 sessions, with continued gains as training progresses.
References and Further Reading
- Levi, D. M., & Li, R. W. (2009). Perceptual learning as a potential treatment for amblyopia: A mini-review. Vision Research, 49(21), 2535–2549. doi:10.1016/j.visres.2009.02.010
- Zhou, Y., Huang, C., Xu, P., Tao, L., Qiu, Z., Li, X., & Lu, Z. L. (2006). Perceptual learning improves contrast sensitivity and visual acuity in adults with anisometropic amblyopia. Vision Research, 46(5), 739–750. doi:10.1016/j.visres.2005.07.031
- Polat, U., Ma-Naim, T., Belkin, M., & Sagi, D. (2004). Improving vision in adult amblyopia by perceptual learning. Proceedings of the National Academy of Sciences, 101(17), 6692–6697. doi:10.1073/pnas.0401200101
- Huang, C. B., Zhou, Y., & Lu, Z. L. (2008). Broad bandwidth of perceptual learning in the visual system of adults with anisometropic amblyopia. Proceedings of the National Academy of Sciences, 105(10), 4068–4073. doi:10.1073/pnas.0800824105
- Levi, D. M., Song, S., & Pelli, D. G. (2007). Amblyopic reading is crowded. Journal of Vision, 7(2), 1–17. doi:10.1167/7.2.21
- Astle, A. T., Webb, B. S., & McGraw, P. V. (2011). Can perceptual learning be used to treat amblyopia beyond the critical period? Ophthalmic and Physiological Optics, 31(6), 564–573. doi:10.1111/j.1475-1313.2011.00856.x
- Hess, R. F., Thompson, B., & Baker, D. H. (2014). Binocular vision in amblyopia: structure, suppression and plasticity. Ophthalmic and Physiological Optics, 34(2), 146–162. doi:10.1111/opo.12123
- Polat, U., Bonneh, Y., Ma-Naim, T., Belkin, M., & Sagi, D. (2005). Spatial interactions in amblyopia: Effects of stimulus parameters and age. Vision Research, 45(11), 1361–1375. doi:10.1016/j.visres.2004.12.005
- Zhang, J. Y., Cong, L. J., Klein, S. A., Levi, D. M., & Yu, C. (2014). Perceptual learning improves adult amblyopic vision through rule-based cognitive compensation. Investigative Ophthalmology & Visual Science, 55(4), 2020–2030. doi:10.1167/iovs.13-13739
- Barry, S. R. (2009). Fixing My Gaze: A Scientist's Journey into Seeing in Three Dimensions. Basic Books.